

Lung ultrasound for the diagnosis of pneumonia in adults: Blue Protocol
- Mazen Kherallah
- Jan 5, 2022
- 2 min read
Updated: Oct 7, 2022
Ultrasound in the intensive care unit is a reasonable gold standard to detect many causes of respiratory failure with a sensitivity and specificity ranging from 90% to 100%. The BLUE-protocol (Bedside Lung Ultrasound in Emergency) was developed at university-affiliated teaching-hospital ICUs in France led by Lichtenstein et al, and is now widely used as a fast and easy tool in the differential diagnosis of acute respiratory failure [1].
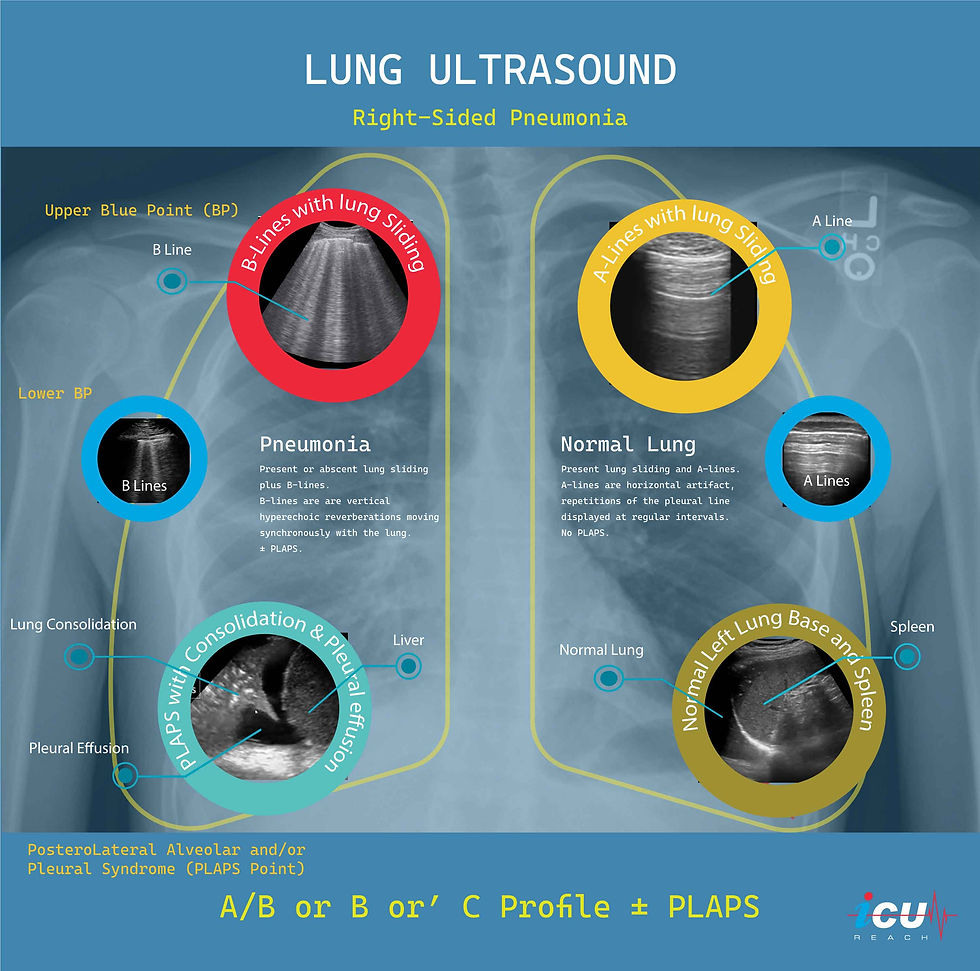
The BLUE-protocol combines ultrasound signs (lung sliding, A lines, B lines, and PLAPS) with location, associated with results of a sequential venous analysis (thrombosed versus free veins) to give a clinical diagnosis and etiology of acute dyspnea and respiratory failure.
Lung sliding is the shimmering movement of the visceral and parietal pleural surface along with respiration.
A-lines are horizontal artifact result from reverberation of the ultrasound beams off the pleura. They occur at equal intervals and indicate dry interlobular septa (normal lung).
B-lines are discrete laser-like (comets) vertical hyperechoic artifacts extending from the pleura to the edge of the screen and indicate a thickened interlobular septa (pulmonary edema or pneumonia).
PLAPS stands for a PosteroLateral Alveolar and/or Pleural Syndrome representing lung consolidation/collapse and/or pleural effusion.
The combination of these signs results in seven different profiles:
A-profile combines anterior lung-sliding with A-lines bilaterally.
A’-profile when A-lines are present bilaterally with abolished lung-sliding.
B-profile associates anterior lung-sliding with lung-rockets bilaterally.
B’-profile is B-profile with abolished lung-sliding.
C-profile indicates anterior lung consolidation (any size and number) or a thickened, irregular pleural line.
The A/B profile is a half A-profile at one side, a half B-profile at another.
The PLAPS-profile indicates a PosteroLateral Alveolar and/or Pleural Syndrome.
The four profiles that can indicate the presence of pneumonia are A/B-profile, B’-profile, C-profile, or A-profile with clear veins and PLAPS. Ultrasound lacks sensitivity in detecting pneumonia when these profiles are present individually (11-42%) but their absence has an excellent specificity (96-100%). The presence of a combination of these four profiles gives a sensitivity of 89% and specificity of 94% in the diagnosis of pneumonia.
In the above image, CXR shows right sided infiltrate and ultrasound reveals A/B profile (lung sliding with B-lines on the right side and A-lines with lung sliding on the left side) with PLAPS (consolidation with pleural effusion).
References
Lichtenstein DA, Mezière GA. Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE protocol. Chest. 2008 Jul;134(1):117-25. doi: 10.1378/chest.07-2800. Epub 2008 Apr 10. Erratum in: Chest. 2013 Aug;144(2):721. PMID: 18403664; PMCID: PMC3734893.
Kaiser OTC benefits provide members with discounts on over-the-counter medications, vitamins, and health essentials, promoting better health management and cost-effective wellness solutions.
Obituaries near me help you find recent death notices, providing information about funeral services, memorials, and tributes for loved ones in your area.
is traveluro legit? Many users have had mixed experiences with the platform, so it's important to read reviews and verify deals before booking.