


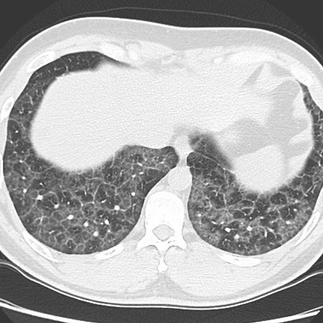
Confirmed influenza pneumonia

Donohue JF et al. Ensifentrine as a novel, inhaled treatment for patients with COPD. Int J Chron Obstruct Pulmon Dis 2023 Jul 28; 18:1611. (https://doi.org/10.2147/COPD.S413436)
Population:
Patients with moderate-to-severe Chronic Obstructive Pulmonary Disease (COPD).
Approximately 1500 participants involved in the trials (ENHANCE-1 and ENHANCE-2).
Intervention:
Administration of Ensifentrine (Ohtuvayre), a novel phosphodiesterase 3 and 4 inhibitor, via nebulizer.

Early home discharge in low-risk PE patients, as identified by validated triage tools (sPESI and Hestia), is safe with very low incidences of adverse events and mortality. However, patients with cancer, elevated troponin, or elevated NT-proBNP have a higher risk of adverse events and may require closer monitoring.
Safety of treating acute pulmonary embolism at home: an individual patient data meta-analysis | European Heart Journal | Oxford Academic (oup.com)

Medical Devices Visible:
1. Endotracheal Tube (ETT)
2. Central Venous Catheter
3. Chest Tubes
4. ECG Leads
A 42-year-old man with progressive cough, fever, and shortness of breath for three weeks. Here are the key points and findings:
Medical Conditions: Hyperlipidemia and hypertension.
Medications: Atorvastatin 20 mg daily, lisinopril 10 mg daily.
Lifestyle: Non-smoker.
Recent Activity: Recently placed mulch in his yard.
42-year-old man with progressive cough, fever, and shortness of breath for three weeks. He recently placed mulch in his backyard.
Medical Conditions: Hyperlipidemia and hypertension.
Medications: Atorvastatin 20 mg daily, lisinopril 10 mg daily.
Lifestyle: Non-smoker.
Recent Activity: Recently placed mulch in his yard.


Symmetric diffuse, bilateral pulmonary infiltrates with mediastinal and bilateral hilar lymphadenopathy. DDx?

What do you want to do next?
Thank you, in addition to the pneumomediastinum and SQ emphysema, there is also a pneumothorax on the right side and a chest tube is needed since this patient is on the ventilator. @Everyone
Determining CD4+/CD8+ ratio can be helpful in the diagnosis of sarcoidosis. Sarcoidosis is characterized by an increased CD4/CD8 ratio (>3.5), compared with other interstitial lung diseases.

A 57-year-old sarcoidosis patient is showing "cobblestone" appearance in the endobronchial Biopsy proved multiple non-necrotizing granulomas.

Löfgren syndrome is a type of acute sarcoidosis an inflammatory disorder characterized by swollen lymph nodes in the chest, tender red nodules on the shins, fever and arthritis.

Heerfordt syndrome, or uveoparotid fever, occurs in 10% of cases and consists of a triad of parotid enlargement, uveitis, and seventh cranial nerve palsy

This figure shows three consecutive FDG-PET performed in a patient with progressively more aggressive therapy for sarcoidosis.

Bilateral apical pneumothoraces, approximately 10% in size on the right and 20-30% on the left without mediastinal shift with diffuse alveolar infiltrates and air bronchograms.
The lung is anatomically divided into smaller units known as lobules, which are the smallest functional units of the lung visible to the naked eye. Each lobule is roughly hexagonal in shape and is bounded by connective tissue septa. Within these lobules, the lung's essential structures for gas exchange are contained, including terminal bronchioles, respiratory bronchioles, alveolar ducts, and alveoli. The terminal bronchiole, which is the smallest airway without alveoli, branches into several respiratory bronchioles, marking the transition where gas exchange begins. Blood supply to the lobules is via the pulmonary arteries and veins traveling through septa and branching along the bronchioles. Lymphatic vessels within the lobules help to maintain fluid balance and remove debris.
The "crazy paving" pattern on chest HRCT or standard CT refers to the appearance of ground-glass opacities with superimposed interlobular and intralobular septal thickening. This pattern is named for its resemblance to irregularly laid paving…
A 24-year-old woman is evaluated for intermittent cough, wheezing, and chest tightness of 1 month's duration. She reports worsening symptoms with exercise and with cat exposure.
On physical examination, vital signs are normal. She has end-expiratory wheezing. Cardiac examination is normal.
On spirometry, FEV1 is 75% of predicted and improves significantly following inhaled albuterol.
Which of the following tests will help predict this patient's responsiveness to glucocorticoids?
0%Bronchial Challenge Test
0%Diffusing Capacity for Carbon Monoxide
0%Pulse Oximetry
0%Fractional Exhaled Nitric Oxide
Fractional exhaled nitric oxide (FeNO) will help predict this patient's responsiveness to inhaled glucocorticoids. Although FeNO should not be used as a diagnostic tool for asthma, it can be used to support this diagnosis in situations in which additional objective evidence is needed. FeNO may be useful if there is uncertainty in choosing, monitoring, or adjusting anti-inflammatory therapies based on history, clinical findings, and spirometry as part of an ongoing asthma monitoring and management strategy. In adults with respiratory symptoms, FeNO levels above 50 ppb correlate with eosinophilic airway inflammation and predict response to inhaled glucocorticoids. FeNO levels below 25 ppb indicate that eosinophilic airway inflammation and glucocorticoid responsiveness are less likely; values between 25 and 50 ppb should be interpreted cautiously. In patients with asthma that is being treated with inhaled glucocorticoids, serial measurement of FeNO may help to monitor patient response to glucocorticoid therapy.
Bronchial challenge testing is used to identify bronchial hyperresponsiveness, a diagnostic feature of asthma. This is particularly helpful in patients whose symptoms are suggestive of asthma but for whom other pulmonary function test results are normal. Patients inhale increasing doses of a substance known to induce bronchospasm, such as methacholine or histamine, in a stepwise fashion. This is followed by repeated measurements of FEV1; if FEV1 falls by 20% or more from the baseline value, the test is considered positive.
Diffusing capacity for carbon monoxide (DLCO) measurement estimates the amount of gas transfer through the alveolar/capillary unit and is proportional to the surface area of a functional lung. DLCO is measured by inhalation of a gas mixture containing carbon monoxide and helium; the resulting value is corrected for hemoglobin level. DLCO is reduced in conditions in which functioning alveolar capillary units are destroyed, infiltrated, removed, or their function is compromised. Conditions that increase pulmonary capillary blood volume, such as pulmonary alveolar hemorrhage, left-to-right shunt, or asthma, can cause an elevation in DLCO. DLCO measurements do not predict responsiveness to glucocorticoids.
Pulse oximetry provides a readily available noninvasive measurement of oxygen-bound hemoglobin in the circulation. A normal hemoglobin saturation measured by pulse oximetry is 95% to 100%, and values below 90% indicate hypoxemia. Pulse oximetry cannot predict responsiveness to glucocorticoids.
Spot Diagnosis??
@Nader Guma you may want to give hints and orientation so we get some engagement!

What radiological sign would describe this appearance on the CT of this patient and what is the significance of this sign?

This is from NEJM image of the week at:
A 28-year-old woman presented to the hospital with a 6-month history of dry cough. She was a lifetime nonsmoker and reported having no fevers, joint aches, eye pain, or rashes. On physical examination, auscultation of both lower lungs revealed fine crackles. High-resolution computed tomography (CT) of the chest showed mediastinal lymphadenopathy and diffuse ground-glass opacities (Panel A, axial view). Also visible were areas of superimposed interlobular and intralobular septal thickening, a pattern known as crazy paving because of the resemblance to irregular paving stones (Panel A, box). The serum level of angiotensin-converting enzyme was 80 U per liter (reference range, 17 to 55). A subsequent transbronchial lung biopsy showed multiple noncaseating granulomas (Panel B, inset showing granuloma; hematoxylin and eosin stain). Bronchoalveolar-lavage cultures, histopathological analysis, and molecular testing were negative for infectious organisms, including Mycobacterium tuberculosis. A diagnosis of pulmonary…


This is a screenshot of the case that Dr. @Nader Guma posted earlier, please review the case and the share with the group the best approach in the management of this case.
Here is the link to the case:
https://www.mobileapp.app/to/MLFUpmu?ref=2_cl
I would advise for (check all what apply):
0%Catheter-directed embolectomy
0%Catheter-directed thrombolysis
0%Systemic anticoagulation
0%Surgical embolectomy
You can vote for more than one answer.
The best choice for this patient with tumor embolism is to do surgical embolectomy to avoid fragmentation of the embolus causing pulmonary tumor emoboli if catheter-directed embolectomy is chosen. In addition, all patients should placed on anticoagulantion as these tumor embolism are thrombogenic and likely to be associated with thrombosis.
@Everyone
47 year old male with no significant PMHx who presented to ED c/o chest pain and sob x 12h
As a part of ED work up they ordered stat TTE I did his echo and as everyone can see a large mobile echogenic mass (measuring ~ 5-6 x 2 cm) moving in-and-out of the tricuspid annulus, most likely representing thrombus/emboli in transit.
Final diagnosis was
PE in patient with RCC
occur due to tumors emboli from the involvement of the IVC with local tumor extension
This is a 26 yo M with history of obesity and asthma, who is presenting with shortness of breath x3 days, tested positive for influenza A, started on bilevel oxygenation for respiratory distress. Patient was noted to feel more short of breath and complain of neck swelling. CT as above.
What is your diagnoses(s)?
How would you manage this patient with these new findings?
@Everyone
A nice narrative review of Pneumomediastinum and pneumothorax in ARDS

Only by the images, what do you think this is?

Diagnosis?
@Everyone
How would you classify the case knowing that the patient has tachycardia at 110 with stable blood pressure, troponin and BNP are elevated?
@Everyone
A 62-year-old man comes to the emergency department after "coughing up a 6-ounce cupful of blood." He describes about 3 days of increased yellowish sputum production associated with mild increase in dyspnea on exertion. On the previous 2 days he had slight blood streaking in the sputum. He has no prior history of hemoptysis. He has no fever, chills, weight loss, or night sweats.
His past medical history is significant for HIV and tuberculosis treated 12 years ago with directly observed therapy for 9 months. He is compliant with highly active antiretroviral therapy. He is an ex-IV drug user with a 50-pack-year history of tobacco use.
On examination, the patient is very anxious appearing with mild respiratory distress and some dried blood on his lips.
Pulse is 104/min, respirations are 20/min, and SaO, is 90% on room air. Lung examination shows mild diffuse wheezing. He coughs up an additional 25…
The Monod sign refers to the presence of gas surrounding a mycetoma, typically an aspergilloma, within a pre-existing pulmonary cavity. It is a distinct radiographic feature indicating a freely mobile mass within the cavity that can move when the patient's position changes, optimally observed when images are acquired in a prone position to allow the mass to shift to a gravity-dependent location. This sign should not be confused with the air crescent sign, which is associated with the recovery phase of angioinvasive aspergillosis and indicates an improvement in the patient's condition. Despite the specific implications of the Monod sign, in clinical practice, the term is not widely recognized, and the gas pattern around the mycetoma is often crescent-shaped. Consequently, the term air crescent sign is frequently used interchangeably to describe both phenomena, although they represent different pathological processes.
@Everyone
A 72 y/o male with a PMH of gout and hyperlipidemia presents to the clinic for chronic persistent cough, dyspnea on exertion and a 50 lb weight loss over the past 4 months.
His cough is mostly dry and reports no recent URTIs/LRTIs. He also complains of night sweats for the past few weeks. He denies having any fevers, headache, blurry vision, chills, N/V, chest pain, palpitations, hemoptysis, orthopnea, diarrhea, constipation, urgency urination or other medical complaints, and has no recent travel history. He has been a professional boxer throughout his life. He stopped training 2 months ago because of his cough and dyspnea.
VSS
Patient appears fatigued and weak. Physical examination is unremarkable.
He is currently not taking any medications.
Thank you @Nader Guma please provide a follow up on the work up that was done and update us once the diagnosis is established

















Bilateral pneumonia