

Your diagnosis?
top of page

Internal Medicine
Public·90 members







Post-obstructive uropathy with acute kidney injury and bilateral severe hydronephrosis secondary to bladder outlet urinary obstruction.


Noor Ali Shah
31 ago
•
The most important approach should be done,
1. Do urgent electrolytes and urea creatinine to rule out hyperkalemia or electrolytes imbalance and renal function status after details history and clinical examination.
2. Do 12 lead ECG and Echo to see cardiac function status.
3. Consult urologist for possible relief of obstruction either insertion of small IFC or supra pubic approach through small incision.
4. Urgent nephrology consultation for possible HD if indicated.
5. Under lying cause should be identified as soon as possible and address accordingly.
Editado
Transjugular Intrahepatic Portosystemic Shunt (TIPS) in Portal Hypertension
Portal hypertension is the increased blood pressure within the portal venous system, which can lead to serious complications like variceal bleeding, refractory ascites, and hepatic hydrothorax. TIPS reduces portal hypertension by diverting a portion of the portal blood flow directly into the systemic circulation, thereby decreasing the pressure in the portal venous system
The key indications include recurrent variceal bleeding that is unresponsive to endoscopic or pharmacological treatments, refractory ascites that does not respond to diuretics or repeated paracentesis, and hepatic hydrothorax resistant to medical therapy. Additionally, TIPS may be used in managing Budd-Chiari syndrome, where thrombosis of the hepatic veins leads to increased portal pressure.


Aphthous stomatitis!
Noor Ali Shah
19 ago
•
Aphthous stomatitis, or recurrent aphthous stomatitis, commonly referred to as a canker sore, is a common condition characterized by the repeated formation of benign and non-contagious mouth ulcers in otherwise healthy individuals.
It is also called Canker sore. It is painful and irritating. It’s more common in female than male. It is usually benign in origin.
Common causes of simple sore
Stress,
Acidic food use,
Injury to mucous membranes,
Dental appliances such as braces,
NSAID use.
While complex sores are common in immune compromised patients.
Treatment is just apply anaesthetic gels and usually healed in 1-3 weeks without scarring. Occasionally used topical antibiotics or steroids for treatment . Nutritional deficiencies should be corrected such as B-12 etc. Avoid trigger food items.
Editado

Wegdan Abdalla
14 ago
•
Medical Devices Visible:
1. Endotracheal Tube (ETT)
2. Central Venous Catheter
3. Chest Tubes
4. ECG Leads

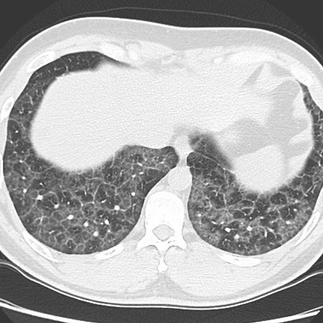
Your diagnosis?






Symmetric diffuse, bilateral pulmonary infiltrates with mediastinal and bilateral hilar lymphadenopathy. DDx?

What do you want to do next?
Mazen Kherallah
15 may
Thank you, in addition to the pneumomediastinum and SQ emphysema, there is also a pneumothorax on the right side and a chest tube is needed since this patient is on the ventilator. @Everyone

Large peripancreatic retroperitoneal fluid collections with gas formation representing necrotizing pancreatitis.
80-year-old male who had a second- and third-degree burn injury was found to have an automated platelet's count of 980,000 while a manual analysis revealed it is 165,000. This is a heat-induced fragmentation of RBCS causing a false automated reading of the platelets.




Probe location (zone L3): 4th-10th intercostal spaces, between the anterior & posterior axillary lines.

Transducer Type & Placement
Phased Array or Curvilinear
The footprint is perpendicular to the skin with the marker pointing cephalad

Lung Sliding
Pleural line is found below the chest wall
Movement of pleura with breathing will generate the “lung sliding” sign
• Represents the sliding of the visceral pleura against the parietal pleura
• Using Color Flow (CF) can help identify the pleural line and its movement

Bat Sign: This sign is formed by the shadows of two ribs and the pleural line (looks like a bat flying towards you)

Comet Tail Artifact/B Lines
• Vertical lines, extending from the pleural line to the edge of the screen without fading
• Synchronized with lung sliding
• When present they will usually overshadow the A lines
• Represents thickening interlobular septa and extravascular lung water as in alveolar interstitial disease (pulmonary edema, ARDS...)

A Lines
Can be part of the normal lung signs
Represents normal artifact repetition(s) of the pleural line
Intervals between the A lines are equal to the distance between the skin and the original pleural line
When present without lung sliding, it may indicate the presence of pneumothorax
Radiography of fungal pneumonia

A, Right upper lobe nodule with surrounding ground-glass opacities (halo sign) in a patient with invasive aspergillosis. B, Diffuse ground-glass opacities in a patient with Pneumocystis pneumonia. C, Diffuse ground-glass opacities and scattered thin-walled pneumatoceles in a patient with Pneumocystis pneumonia. D, Peripheral small cavitary nodules in a patient with Candida endocarditis and septic emboli to the lungs.

What is your diagnosis?
0%Rheumatoid arthritis
0%Cirrhosis
0%Amyloidosis
0%Psoriasis
Mazen Kherallah
17 mar

@Everyone You probably were concentrating on the scaling but what about the splinter hemorrhage and the petechiae as indicated by the black arrows, you can change your diagnosis if you wish!




Notice the structure and the abnormality indicated by the yellow arrow and give your diagnosis. @Everyone
Mazen Kherallah
16 mar
Thank you @Tarek Slibi
The structure is an IVC filter and there is a cylindrical clot formed above the filter!
Large areas of cytotoxic edema involving the bilateral cerebral hemispheres and right cerebellum consistent with acute or subacute ischemia associated with sulcal effacement and edema without significant midline shift.






Compare this to her normal CT of head few days ago:

The lung is anatomically divided into smaller units known as lobules, which are the smallest functional units of the lung visible to the naked eye. Each lobule is roughly hexagonal in shape and is bounded by connective tissue septa. Within these lobules, the lung's essential structures for gas exchange are contained, including terminal bronchioles, respiratory bronchioles, alveolar ducts, and alveoli. The terminal bronchiole, which is the smallest airway without alveoli, branches into several respiratory bronchioles, marking the transition where gas exchange begins. Blood supply to the lobules is via the pulmonary arteries and veins traveling through septa and branching along the bronchioles. Lymphatic vessels within the lobules help to maintain fluid balance and remove debris.






The "crazy paving" pattern on chest HRCT or standard CT refers to the appearance of ground-glass opacities with superimposed interlobular and intralobular septal thickening. This pattern is named for its resemblance to irregularly laid paving…





Spot Diagnosis??
Mazen Kherallah
08 mar
@Nader Guma you may want to give hints and orientation so we get some engagement!
Left Ventricular Thrombus
I used ultrasound-enhancing agent (DEFINITY)

bottom of page
Intravenous drug abuse and tricuspid valve endocarditis lead to Multiple cavitary lung lesions (Multiple Lung Abscesses )