

NEJM
May 1, 2014
A Randomized Trial of Protocol-Based Care for Early Septic Shock.
Mazen Kherallah
Summarized by:
What was the research question?
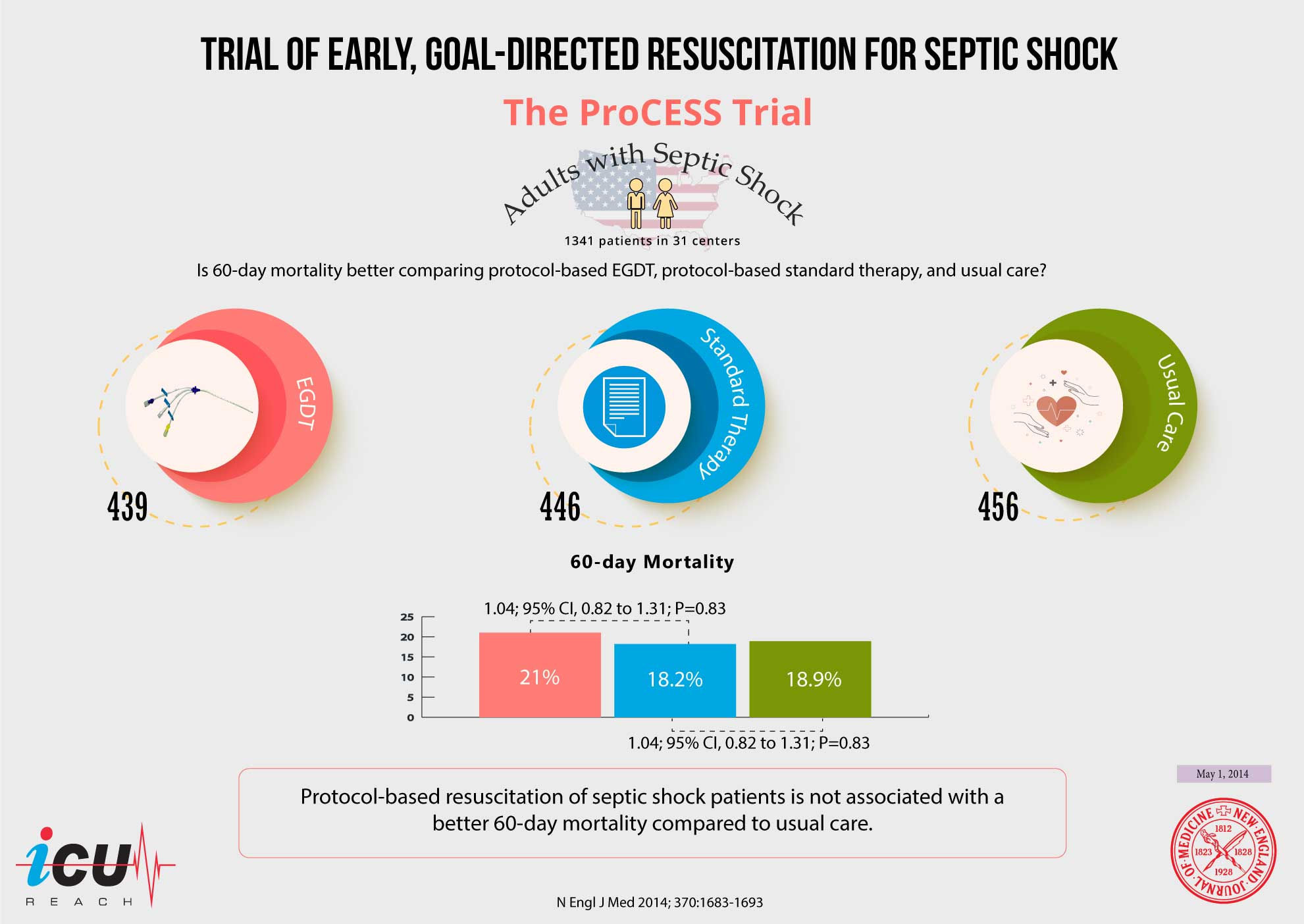
Is 60-day mortality better comparing protocol-based EGDT, protocol-based standard therapy, and usual care in adult patients with septic shock?
How did they do it?
A pragmatic randomized trial in 31 emergency department in the United States.
1341 patients with septic shock were randomly assigned in a 1:1:1 ratio to protocol-based EGDT (439), protocol-based standard therapy (446), or usual care (456) for 6 hours of resuscitation.
Protocol-based EGDT was the Rivers 2001 protocol, which included a central line with SCvO2 monitoring, fluids, vasopressors, dobutamine, and pRBCs. Protocol-based standard therapy did not require the placement of a central venous catheter, administration of inotropes, or blood transfusions in contrast to EGDT. Usual care did not prompt he physician for any treatment.
The primary end point was 60-day in-hospital mortality and whether protocol-based care (EGDT and standard-therapy groups combined) was superior to usual care and whether protocol-based EGDT was superior to protocol-based standard therapy.
Secondary outcomes included longer-term mortality and the need for organ support.
What did they find?
60-day in-hospital mortality was not different for the protocol-based EGDT group (21%), protocol-based standard-therapy group (18.2%), or usual care group (18.9%).
There was no difference in primary endpoint between the combined protocolized patients and usual care (19.5 vs 18.9, p=0.83).
Relative risk with protocol-based therapy vs. usual care is1.04; 95% confidence interval [CI], 0.82 to 1.31; P=0.83. Relative risk with protocol-based EGDT vs. protocol-based standard therapy is 1.15; 95% CI, 0.88 to 1.51; P=0.31.
There were no significant differences in 90-day mortality, 1-year mortality, or the need for organ support.
Subgroup analysis, specifically related to severity of illness, was unrevealing for any differences among the groups.
Are there any limitations?
Not powered to detect any benefit in subgroups.
In-hospital mortality is affected by different physician’s approaches to end of life.
What does it mean?
Protocol-based resuscitation septic shock patients is not associated with a better 60-day mortality compared to usual care.
Usual care has improved over the years since EGDT in providing adequate fluid resuscitation and early antibiotic therapy.
The trial offers a less invasive and equally effective approach to septic shock patients.